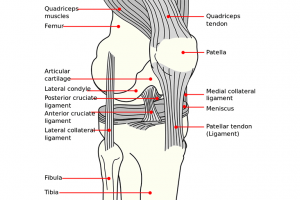
The Anterior Cruciate Ligament (ACL) is one of the four main ligaments that connect the femur to the tibia. The knee is a hinged joint held together by the lateral collateral (LCL), posterior cruciate (PCL), medial collateral (MCL), and anterior cruciate (ACL) ligaments. The ACL runs diagonally in the knee’s middle and prevents the tibia from sliding out in front of the femur. It also provides rotational stability to the knee. The ACL is one of the commonly injured ligaments of the knee. In fact, ACL injuries are estimated at 200,000 yearly. ACL reconstructions performed yearly are also estimated at 100,000. Understandably, the incidence of ACL injury is generally higher in individuals who engage in high-risk sports like football, basketball, soccer, and skiing which involves a lot of pivoting. At least 50 per cent of ACL injuries occur in combination with articular and meniscus damage.
Causes
An estimated 70 per cent of ACL injuries are attributed to non-contact mechanisms while the remaining 30 per cent are attributed to direct contact with an object or another player. The injury mechanism is typically associated with deceleration coupled with awkward landing, sidestepping and pivoting manoeuvres, and cutting. Several studies indicate that female athletes have a higher incidence of ACL injury compared to their male counterparts. It has been proposed that this can be the result of differences in muscular strength, neuromuscular control, and physical conditioning.
When an ACL injury occurs, patients often experience swelling and pain immediately. The knee can also feel unstable and the patient cannot bear weight immediately. Within a few hours after an ACL injury, other symptoms can manifest including loss of full motion range, tenderness along the joint line, and discomfort when walking.
Diagnosis
Aside from special tests to check for meniscus tears and other injuries to the ligaments, the Lachman’s and pivot-shift tests will also be done to check if the ACL is still intact. When checking patients with an ACL injury, an X-ray may also be ordered to check for possible fractures or ligament-bone avulsions. A magnetic resonance imaging (MRI) scan may also be required to assess the ACL and check for evidence of injury to the articular cartilage, meniscus cartilage, and other knee ligaments.
Surgical Treatment
Surgical intervention is often recommended when dealing with combined injuries (ACL tears combined with other knee injuries). Generally, ACL tears are not repaired through suturing since it has been shown to have a high failure rate over time. A torn ACL is generally replaced by a substitute graft (made of a tendon or preferably ligament). Some of the key goals of ACL reconstruction surgery include restoring the torn ligament’s function, creating a stable knee, and preventing instability. If a meniscus tear is repaired, the concomitant ACL tear is also reconstructed.
Patient Considerations
Surgical treatment is encouraged for those patients who are involved in jobs or sports that require hard-cutting, turning, pivoting, and heavy manual work. In adolescents or young children with ACL tears, early ACL reconstruction can put them at risk for growth plate injury which can result in bone growth disturbance.
That being said, it is likely for the surgeon to delay the ACL surgery until the patient is closer to skeletal maturity. The surgeon may also modify the ACL surgery technique to minimize the risk of growth plate injury. ACL surgery is also often recommended for patients who experience significant functional instability and those with torn menisci since they are more prone to developing secondary knee damage.
Surgical Options
1. Hamstring Tendon Autograft – The semitendinosus hamstring tendon situated on the knee’s inner side is used to create the hamstring tendon autograft for ACL reconstruction. Proponents of the hamstring graft claim fewer problems are associated with harvesting of the graft compared to patellar tendon autograft. It has also been known to have more benefits including:
- Reduced kneecap or anterior knee pain
- Lesser postoperative stiffness
- Faster recovery
- Smaller incisions
2. Patellar Tendon Autograft – In patellar tendon autograft, the middle third of the patient’s patellar tendon along with a bone plug from the kneecap and the shin is used. Considered by some as the “gold standard” for ACL reconstructions, it is often the likely resort for high-demand athletes and those patients whose occupations will not involve a significant amount of kneeling.
3. Quadriceps Tendon Autograft – The quadriceps tendon autograft is often recommended for patients who have had a failed ACL reconstruction. A bone plug from the knee cap’s upper end and the middle third of the patient’s quadriceps tendon will be used. However, since the bone plug is on one side only, the fixation may not be as solid as the patellar tendon graft.
4. Allografts – Allografts are grafts taken from cadavers. These grafts are also recommended for patients who need reconstruction for more than one knee ligament and those who have already failed their ACL reconstruction. Allografts have become increasingly popular since it comes with several advantages including less pain (since graft is not obtained from the patient), smaller incisions, and decreased surgery time. The disadvantage is of persistent synovial reaction and knee discharge as well as late stretching.
Postoperative Recovery
Aside from keeping the wound clean and dry, focus is placed on restoring hamstring and quadriceps control and regaining the ability to fully straighten the knee in the first 10 to 15 days after the surgery. Icing the knee regularly is also recommended to minimize pain and reduce swelling. Use of a postoperative brace to help regain the knee’s full-motion range is usually recommended.
After ACL reconstruction, key rehabilitation goals include strengthening the hamstring and quadriceps muscles, maintaining the kneecap’s mobility, regaining the knee’s full-motion range, and minimizing knee swelling. Patients may return to sports when there is no more swelling and pain, when muscle endurance, strength, and functional use of the leg has been restored, and when full motion range of the knee has been achieved. The final steps of physiotherapy are the ability to perform cutting, zig-zag sprints and decelerations without apprehension. This comes through exercises that are designed to improve neuromuscular control.